For the last year, any discussion of the obesity-drug market has come with an asterisk: Everything will change once pill versions of the popular GLP-1 drugs arrive. Those potentially cheaper alternative to injectables could mean a larger slice of the millions of Americans with obesity will try out the medicine.
Just a month into the arrival of the first pill, a version of Novo Nordisk’s Wegovy, and everything really is changing — and fast. The cost of these highly effective medicines is finally coming down from the stratosphere, and in an ideal world, that will help many more consumers afford to use them consistently.
People are clamoring for the pill version of Wegovy, which hit US pharmacy shelves on Jan. 5. Novo told investors this week that more than 170,000 people are already taking the drug. With some 50,000 prescriptions being filled each week, one stock analyst called it the fastest drug launch of all time.
And yet, in the brutally competitive world of obesity medicine, Novo Nordisk’s stock fell by as much as 20% that same day. That’s because the Danish firm also said that its overall sales would fall for the first time in nearly a decade, due to competition and negotiations with the Trump administration to lower the price of Wegovy and its diabetes drug Ozempic.
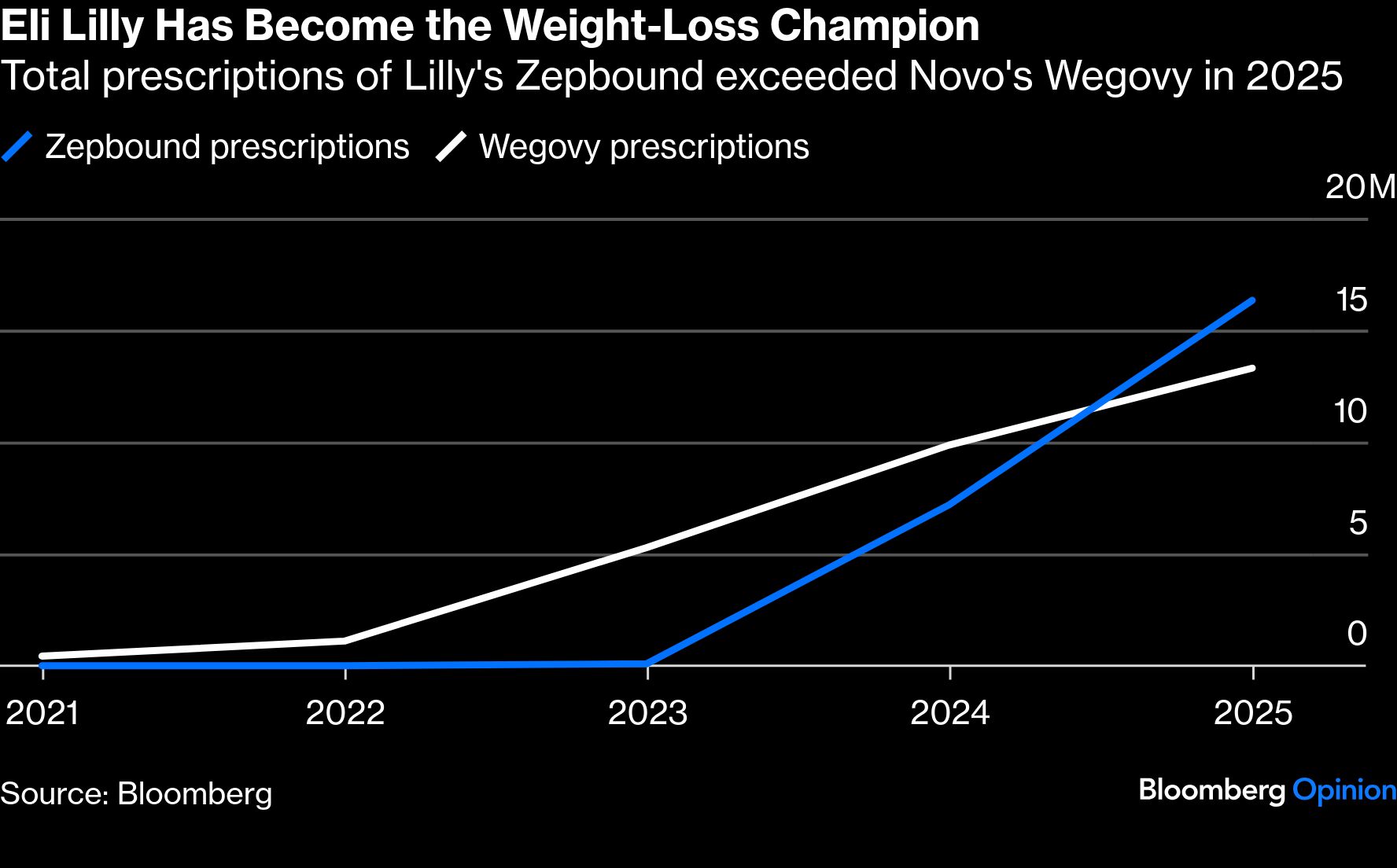
Eli Lilly & Co., on the other hand, cemented its dominance in the market this week by telling investors its revenues will grow by as much as 27% this year. It cited strong demand for its injectable obesity and diabetes drugs, Zepbound and Mounjaro, and the anticipated launch this spring of its own GLP-1 pill, orforglipron.

Novo took another hit a few days later, when telehealth company Hims & Hers said it was launching a compounded version of the Wegovy pill for just $49 per month — $100 cheaper than Novo’s price for the starting doses of its product. The news sent Novo shares tumbling to their lowest level since July 2021, and Lilly’s fell by nearly 9%. (Novo has called the move “illegal.”)
The weeklong drama underscored how quickly oral GLP-1s are shaking everything up — hopefully for the better for consumers who have struggled to consistently access and pay for such medicines.
The pills are giving patients more choices. People who were reluctant or fearful of weekly injections now have an option, and indeed, obesity medicine specialists tell me that most people asking for the pill have yet to try a GLP-1. Meanwhile, the lower cost of the oral drugs could make it easier for people to stick with treatment over the long haul.
That last part is critical. It’s increasingly clear that to reap the vast health benefits of GLP-1s — the weight loss, of course, but more importantly, the lowered risk of heart attacks, strokes, diabetes, chronic kidney disease and more — people will need to take the drugs for years, maybe even for life.
Yet study after study has found that many people quit taking obesity drugs. Last year, research published in JAMA Network Open showed that nearly 65% of people who started a GLP-1 for obesity had stopped taking it within a year. Just over a third of those folks also had restarted treatment again within a year, underscoring the need for more affordable, better tolerated options.
Cost is a major factor in the drop-off. The JAMA study, for example, found that higher-income people were more likely to maintain treatment and to reinitiate it if they quit, suggesting the drugs had simply become unaffordable for some.
That’s no surprise given spotty insurance coverage in the US. Private insurers, feeling strained by high demand for the expensive drugs, have been constantly rejiggering their guidelines for who qualifies them. Medicare, meanwhile, currently only covers the medicines for people with a high body mass index and certain health conditions, such as heart disease or sleep apnea. (The Trump administration recently said that it will allow Medicare to cover the drugs for weight loss alone; however, that isn’t likely to begin until later this year.)
Many consumers have been forced to pay out of pocket for GLP-1s, a situation that can quickly become untenable as people ramp up to stronger, more expensive doses. Novo said this week that cash payments through its own website, telehealth partners and pharmacies accounted for roughly 30% of prescriptions written for injectable Wegovy. Still others have turned to the gray market for compounded versions of obesity medicines, where out-of-pocket costs can be even cheaper, but there’s no guarantee the knock-off products are safe and effective.
For some, the pills might ease the financial burden. Novo charges $149 per month for the starting dose of the Wegovy pill for people paying on their own, a cost that increases to $299 as they go up in dosage. And Novo said this week that “most” of the 170,000 prescriptions written so far for the pill were for people paying cash.
Everything will change again when the next pill arrives. Although the Wegovy pill seems to make people lose slightly more weight, Lilly’s orforglipron has other advantages. In order to be properly absorbed and work its magic, Novo’s drug must be taken on an empty stomach, and patients then must wait another 30 minutes before eating.
Because orforglipron is a small molecule, it doesn’t have those restrictions — and also should be easier and cheaper to manufacture. Lilly already has billions of doses of the pill ready to go once it gets the Food and Drug Administration’s green light and has agreed to sell the lowest dose of the drug to cash-pay customers for $150 per month.
After several years of hand-wringing over the high cost of these groundbreaking medicines, the market is finally evolving to a place where access should be less of an issue. Still, we also should be wary of the enormous shift toward consumers paying for these medicines on their own. As the price comes down, insurers need to take adapt their policies to bring these drugs back into the fold — treating them like every other effective medicine.
A message from Advisor Perspectives and VettaFi: Discover something new! Click here to register for our upcoming webcasts.
Bloomberg News provided this article. For more articles like this please visit
bloomberg.com.
Read more articles by Lisa Jarvis